Referring Providers: Register for our next CE Symposium
The retina lines the interior wall inside the eye, and the vitreous gel fills the main body. When the eye forms, the gel is adherent to the retina's surface, but as a normal aging process, the vitreous begins to degrade and consolidate, causing it to shrink and liquefy. Eventually, this process causes the vitreous gel to separate from the retina and form a posterior vitreous detachment (PVD). Tears in the retina occur when the vitreous gel pulls too strongly on an area of a weakened retina or in an abnormally adherent area. It is typically far in the peripheral retina if a tear occurs and will not affect the vision. However, fluid can migrate through the opening and cause the retina to separate and detach from the eye wall. Retinal detachments cause vision loss and require surgery to treat. If the retinal tear is identified early, it can be treated to prevent a retinal detachment.
As the vitreous gel separates from the retina, it can pull on the retina, causing stimulation experienced as a flash of light, like a spark or lightning strike. When the vitreous gel consolidates and separates from the retina, it can cause a shadow seen as a floater. The new onset of flashes and floaters can indicate an active vitreous detachment and warrants a complete, dilated examination to ensure the retina has not been damaged. If the retina is torn, there may be no other symptoms. Still, if fluid migrates through a retinal tear, it will cause the retina to separate from the eye wall and detach and start with a decrease in peripheral vision with the appearance of a veil or shadow. As the detachment progresses, the shadow can progress from peripheral to central and eventually take up the entire visual field.
The vitreous separation from the retina is an age-related process that almost everyone will experience, making most people at risk of developing a retinal tear or detachment. Most people do not have any symptoms, and the process goes unnoticed. There is a 10-12% chance of having an associated retinal tear with flashes and floaters. If the eye is highly nearsighted or myopic, has had prior surgery, undergone trauma, or has a family history of a retinal tear or detachment, the risk is higher. Since the risk is related to how the eye was made and aging, not much can be done to reduce the risk of developing a retinal tear or detachment. Having a thorough, dilated exam can identify areas of the retina that may be at higher risk and may benefit from prophylactic treatment.
To treat a retinal tear, laser photocoagulation is performed to burn the retina around the opening of the tear; the burn will scar and seal the retina, preventing fluid from migrating through and detaching the retina. Immediately after the laser procedure, the retina does not have additional strength; only after the laser burn starts to scar does the seal form. The laser scar has full strength in the retina at 10-14 days. During this time, the retina is still at risk of detaching, though every day, the risk decreases as the scar develops, increasing strength. It is advised to avoid strenuous and vigorous activity to minimize the risk of developing a retinal detachment.
Surgery is required to repair a retinal detachment, and there are several procedures commonly used: scleral buckle, pars plana vitrectomy, and pneumatic retinopexy.
Scleral buckle surgery has been widely used since the 1950s. In this procedure, a silicone band is placed around the outside of the eye to indent the wall of the eye toward the retina. This provides the retina a solid foundation to reattach to and relieves any potential traction on the retina. Scleral buckle surgery can be performed by itself or combined with a pars plana vitrectomy. When performed alone, cryotherapy is applied to the eye wall beneath the retinal tear to freeze the tissue. This freezing causes a scar to form to permanently adhere the retina to the wall of the eye and seal the retinal tear.
Pars plana vitrectomy involves small incisions made in the eye wall and using a microscope for viewing. Tiny instruments are used to remove the gel in the eye. Careful attention is paid to removing all vitreous traction from the retinal tear. Once the gel is removed, the retina is flattened, and then laser photocoagulation is applied around the retinal tear. This laser burns the retina and will form a scar that permanently seals the retina.
A gas bubble is placed inside the eye to hold the retina in place while the scar is forming. To properly position the gas bubble and keep the retina in place, it is vital to have the head in the face-down position. Positioning may be required up to 2 weeks after surgery, depending on the damage to the retina. The gas bubble will be resorbed over time and replaced with the eye’s natural fluid but can take up to 2 months to completely resolve. During this time, it is very important to avoid air travel, high altitudes, and nitrous oxide anesthesia as these can cause an increase in the size of the gas bubble, resulting in elevated eye pressure and potentially vision loss. If the retina requires more support than the gas bubble can offer or if there is a need for air travel, a silicone oil bubble can be used. The oil has the same function as the gas, to hold the retina in place during healing. After the retina has healed and stabilized, another surgery removes the oil. Depending on the damage, the silicone oil may be left indefinitely to support the retina.
Pneumatic retinopexy is an office-based procedure during which a gas bubble is injected into the eye to seal the retinal tear. After sterilizing the eye's surface, a small bubble of gas is injected into the eye, and the head is positioned so that the bubble will float to cover the retinal tear. Once the tear is covered, the fluid can absorb and flatten the retina back to the wall of the eye. When the retina has flattened, cryotherapy or laser photocoagulation can be applied to seal the retinal tear. The head must maintain position until the scar tissue forms completely. Proper positioning is essential for the success of the procedure.
Each procedure has specific advantages and disadvantages and can be used alone or in combination to repair retinal detachments.
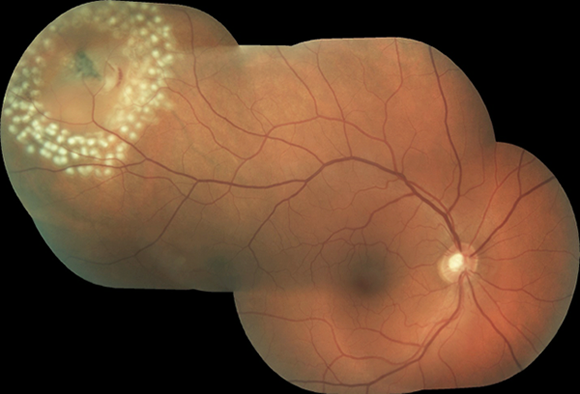
Laser Retinopexy burns the retina around the tear to form a scar that seals the retina in place
After successful reattachment surgery, the visual recovery is variable. The most important factor is if the central retina, the macula, is detached. Some cells will have permanent damage that cannot be repaired when the retina detaches, while others will improve after reattachment. The majority of the recovery happens during the first month, but the vision can improve for up to 1 year after surgery.
Request an appointment now